Preimplantation Genetic Diagnosis (PGD) now termed Preimplantation Genetic
Testing (PGT) is the earliest form of prenatal diagnosis. A single cell or a few cells are removed (biopsied) from the embryo obtained using IVF technology and checked for specific genetic abnormalities. The embryos that are reported normal are transferred into the mother’s uterus. PGT offers a new alternative to chorionic villus sampling or amniocentesis. PGT testing requires multiple embryos developed by ICSI.
(A) PGT FOR ALL 24 CHROMOSOME ANEUPLOIDIES (PGS OR PGT-A) Preimplantation Genetic Screening (PGS), also called Preimplantation Genetic Testing for Aneuploidy (PGT-A), checks for the number of chromosomes and any major gain or loss of genetic material in the chromosomes.
What are chromosomes?

Chromosomes which are present in the nucleus of the cell, contain the genetic material of the cell. Chromosomes contain DNA. Our DNA is organized into small structures called genes. These influence our growth and development. Genes are transmitted from parent to offspring and are considered to be the basic units of inheritance.
Forty-six chromosomes are present in all human cells except the gonadal cells (eggs and sperm). The egg and the sperm each have 23 chromosomes, of which 22 are autosomes, and 1 is the sex chromosome. In the egg, the sex chromosome is always X. In each sperm, the sex chromosome can be either X or Y. When the egg and sperm unite at fertilization, the number of chromosomes becomes 46. Depending on which sperm fertilises the egg, the embryo becomes male (XY) or female (XX).
In each embryo, chromosomes 1 to 22 are in 2 copies, where one comes from the sperm (biological father) and the egg (biological mother). Thus, an embryo with 46 chromosomes (22 pairs of autosomes and one pair of sex chromosomes) is considered a euploid (Normal) embryo.
When the number of chromosomes alters, the embryo is aneuploid (Abnormal). Monosomy occurs when there is a loss of 1 copy of the chromosome from the pair. When an extra copy is present, it is called trisomy of that particular chromosome. When the entire set of 23 chromosomes is extra, it is called triploidy. When both sets of 23 chromosomes are extra, it is called tetraploidy. If the copy number is more than 4, it is called polyploidy. If only 1 set of chromosomes (23) is present, it is called haploidy. If more than one cell line is current, one with 46 chromosomes and the other with more or less than 46, it is called
mosaicism. Mosaicism can occur during embryonic division.
Aneuploidies of embryos can result in spontaneous miscarriages, stillbirths, or developmental disorders in children. The most common aneuploidies are of chromosomes 13, 18, 21, X and Y, followed by aneuploidies of chromosomes 16 and 22.
(B) PGT FOR STRUCTURAL REARRANGEMENTS (PGS OR PGT-SR)
A chromosome translocation is a chromosome abnormality caused by the rearrangement of parts of 2 different chromosomes. Translocations can be balanced (an exchange of material with no extra or missing genetic information) or unbalanced (where during the exchange of chromosome material, there can be extra or missing genes, and normal functionality is affected). Couples with balanced translocations have a 25% chance of having a child with normal chromosomal make-up and a 25% chance of having a child with balanced translocation (fully functional). There is a 50% risk of having a child with unbalanced translocation, which may lead to miscarriage, Intrauterine growth restriction (IUGR), Intrauterine fetal death (IUFD) or
delayed developmental milestones.
(C) PGT FOR MONOGENIC DISORDERS (PGT-M):
Just like chromosomes come in pairs, most genes come in pairs, one from the egg and one from the sperm. When the function of a gene is altered by a change (called a mutation) in the specific sequence of the DNA, a genetic disease results; these mutations can be transmitted in families from generation to generation (inherited) or can be a new change in an individual (de novo). These mutations lead to either single gene or multiple gene disorders.
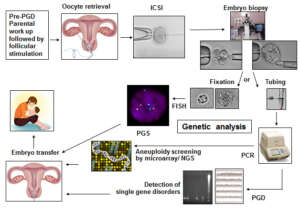
For PGT testing, multiple embryos are developed by performing ICSI. The steps involved in PGT are:
- Pre-PGT work-up:
For the couple opting for PGT for single gene disorders (PGT-M), it is important to carry out Genetic testing for the disorder in both partners prior to PGT-M. This determines the mutation (alteration in genetic material) status of both partners. Based on the genetic report, the actual PGT protocol is developed. PGT for single gene disorders (PGD/PGT-M) is carried out only for the known disorder and mutation which is identified for the couple. Other unknown genetic abnormalities cannot be tested at this time.
Other important genetic tests for PGT/PGD/PGS:
- Karyotyping: Chromosomal analysis is carried out to check for aneuploidy, translocation or the presence of mosaicism.
- Sperm FISH to check for a percentage of aneuploid sperm. (i.e. sperm with an abnormal number of chromosomes)
- Sperm DNA Fragmentation Index to check for the percentage of sperm with DNA fragmentation.
Many routine blood parameters are also tested. Once these reports are ready, the ovarian stimulation cycle begins.
- Hormonal stimulation and oocyte retrieval: The female partner undergoes ovarian stimulation using hormones in order to obtain an adequate number of eggs. The eggs are collected under mild anesthesia.
- ICSI/ IMSI: ICSI (Intracytoplasmic sperm injection) is performed. A single sperm is injected into the
cytoplasm of the mature egg. After fertilization, the embryo is further incubated in culture up to Day 5/Day 6/Day 7.
- Embryo biopsy at the Blastocyst stage: For chromosomal aneuploidy screening (PGS / PGT-A) and for single-gene disorders (PGD / PGT-M), the embryo biopsy is done on Day 5 or Day 6 (Blastocyst Stage).
The Blastocyst is made up of a cluster of cells called the Inner Cell Mass (ICM): which forms the fetus and the trophectoderm cells (which form the placenta). By gentle micromanipulation about 5-8 trophectoderm cells are aspirated into a pipette, loaded into a tube and sent for genetic analysis.

All of the above steps are carried out in the Embryology Laboratory. The trophectoderm cells are then transported to the Genetics Lab for further testing. After the biopsy, the embryos are cryopreserved till the day of embryo transfer.
▪ Different techniques of genetic testing include Fluorescence in Situ Hybridization (FISH), Array Comparative Genomic Hybridization (aCGH) and Next Generation Sequencing (NGS).
▪ Embryo transfer of the genetically normal embryos is carried out in a frozen embryo transfer (FET) cycle and sometimes in the same cycle by doing a quick run analysis.
▪ A pregnancy test is performed 14 days later.