We have an ongoing program for Oocyte donation for women with premature ovarian failure.
The donors are physically, medically and genetically screened. This is one of the most comprehensive and reliable Donor Eggs and Donor Embryo Program in India.
 This oocyte donation program is also suitable for women with poor ovarian reserve, surgical or induced menopause and those in the perimenopausal group. Some women with repeated decreased recruitment of follicles at the time of IVF, poor quality of oocytes, high FSH, low AMH, with extensive endometriosis, severe pelvic adhesions and inaccessible ovaries can also avail of this facility.
This oocyte donation program is also suitable for women with poor ovarian reserve, surgical or induced menopause and those in the perimenopausal group. Some women with repeated decreased recruitment of follicles at the time of IVF, poor quality of oocytes, high FSH, low AMH, with extensive endometriosis, severe pelvic adhesions and inaccessible ovaries can also avail of this facility.
Egg donors are carefully screened and matched with recipients as closely as possible by physical characteristics. They are also screened for sexually transmitted diseases. In case of a genetic mutation in the male partner of the couple seeking Egg Donation, the Oocyte Donor is screened for a similar mutation so that the genetic disease is not passed on to the offspring. We ensure complete confidentiality and evaluate the background of the donors thoroughly. Donors also undergo a genetic test called Karyotyping in order to ensure that they have normal chromosomes. The family background of the donors is checked for genetic diseases. Advanced genetic testing is done as required. We follow ICMR guidelines for our Donor Egg Programme. Donors undergo whole exome analysis to look for any pathological variants, i.e. Gene Mutations that can be harmful, if they are passed on to the baby. Oocyte donors having such mutations are not included in our program.
In Vitro Fertilization (IVF)
IVF achieves pregnancy by fertilizing the woman’s eggs (oocytes) outside her body. The oocytes are obtained under mild anaesthesia using transvaginal guided Sonographic procedures.
ISOLATION OF OOCYTES
The semen is processed in order to obtain the most healthy sperm. The eggs and sperm are incubated together. Next day, the oocyte is checked for fertilization. The embryos are ready for transfer subsequently. IVF is ideal for couples with tubal blockage or pelvic adhesions, previous tubal sterilization not amenable to reversal and some cases of endometriosis and pelvic factor.
 Prior to implantation, the embryo has to escape out of its protective shell known as the zona pellucida by a process known as Hatching. If this process is not completed properly, implantation will fail and pregnancy will not occur. We offer Laser technology for Assisted Hatching (LAH), where a laser beam is focused over the zona pellucida making a small opening, between 30-40 microns to facilitate embryo hatching. This technique is particularly useful in women where the embryo has a thick zona and also in women with previous failed cycles and older women where the zona tends to be thick. Laser Assisted Hatching is also carried out during the process of Preimplantation Genetic Testing (PGT) where the diode laser is also used to make an opening in the zona through which a cluster of 5-8 cells called Trophectoderm cells are aspirated at the time of PGT. However, selection of this procedure for the right application is important.
Prior to implantation, the embryo has to escape out of its protective shell known as the zona pellucida by a process known as Hatching. If this process is not completed properly, implantation will fail and pregnancy will not occur. We offer Laser technology for Assisted Hatching (LAH), where a laser beam is focused over the zona pellucida making a small opening, between 30-40 microns to facilitate embryo hatching. This technique is particularly useful in women where the embryo has a thick zona and also in women with previous failed cycles and older women where the zona tends to be thick. Laser Assisted Hatching is also carried out during the process of Preimplantation Genetic Testing (PGT) where the diode laser is also used to make an opening in the zona through which a cluster of 5-8 cells called Trophectoderm cells are aspirated at the time of PGT. However, selection of this procedure for the right application is important.
 Our centre utilizes the Diode laser which is the safest laser in ART. The entire procedure is completed in a few milliseconds.
Our centre utilizes the Diode laser which is the safest laser in ART. The entire procedure is completed in a few milliseconds.
We achieved the first pregnancy in India using this technique combined with blastocyst transfer (LAHBT). This facilitates its hatching in the uterus and improves implantation and pregnancy rates. In our published study we have demonstrated pregnancy rates to rise from 19% to 44% in this group of women. (Parikh et al., Indian Journal of Obstetrics and Gynacology. November, 2000.)
When the number of chromosomes alters, the embryo is aneuploid (Abnormal). Monosomy occurs when there is loss of 1 copy of the chromosome from the pair. When there is an extra copy present, it is called trisomy of that particular chromosome. When the entire set of 23 chromosomes is extra, it is called triploidy. When both the sets of 23 chromosomes are extra, it is called tetraploidy. If the copy number is more than 4, then it is called polyploidy. If only 1 set of chromosomes (23) is present then it is called haploidy. If more than one cell line is present where one is with 46 chromosomes and other with more or less than 46, it is called as mosaicism. Mosaicism can occur during embryonic division at any stage.
Aneuploidies of embryos can result in spontaneous miscarriages, stillbirths, or developmental disorders in the newborn. The most common aneuploidies are of chromosomes 13, 18, 21, X and Y, followed by aneuploidies for chromosomes 16 and 22.
A chromosome translocation is a chromosome abnormality due to rearrangement of parts of 2 different chromosomes. Translocations can be balanced (an exchange of material with no extra or missing genetic information) or unbalanced (where the exchange of chromosome material results in extra or missing genes and normal functionality is affected). The couples with balanced translocation have a 25% chance of having a child with a normal chromosomal make-up and a 25% chance of having a child with balanced translocation (they are fully functional). There is a 50% risk of having a child with unbalanced translocation which may lead to miscarriage, Intrauterine growth restriction (IUGR), Intrauterine fetal death (IUFD) or delayed developmental milestones.
What is a Gene disorder?
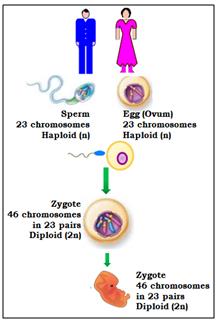
Just like chromosomes come in pairs, most genes also come in pairs, one from the egg and one from the sperm. When, the function of a gene is altered by a change (called a mutation) in the specific sequence of the DNA, a genetic disease results. These mutations can be transmitted in families from generation to generation (inherited), or can be a new change in an individual (de novo). These mutations lead to either single gene or multiple gene disorders.
Genetic diseases can be inherited in different ways. A dominant genetic disease is caused by a mutation in one copy of a gene. The risk for a parent with the disease to pass the condition to the child is 50%. e.g. Huntingtons Chorea.
A recessive genetic disease is caused by a mutation in both copies of a gene. A carrier has one normal copy of the gene and one copy with a mutation. Most of them are healthy since having one normal copy is enough to prevent the disease. Two carrier parents have a 25% risk of having a child with the genetic disease. e.g. Thalassemia, Cystic Fibrosis.
Sex-linked genetic diseases are caused by mutations on the X or Y chromosomes. Sex-linked diseases can be dominant or recessive and affect males and females differently. In some genetic diseases, the abnormality in the gene keeps increasing in the next generation and its expression is seen only when an affected child is born. e.g. Fragile X Syndrome. Hence, if there is any history of having an affected child, it is advisable to undergo testing for the next pregnancy and also test the other family members.
Preimplantation Genetic Testing is carried out for couples who are at a high risk for various genetic disorders, those with male factor, in advanced maternal age or repeated failed IVF. PGT-M is also done for genetic conditions such as Thalassemia, Sickle Cell Disease, Duchenne Muscular Dystrophy, Leigh Syndrome, Huntington Disease, Neurofibromatosis, Cystic Fibrosis and in Hereditary Cancer Predisposition Syndromes.
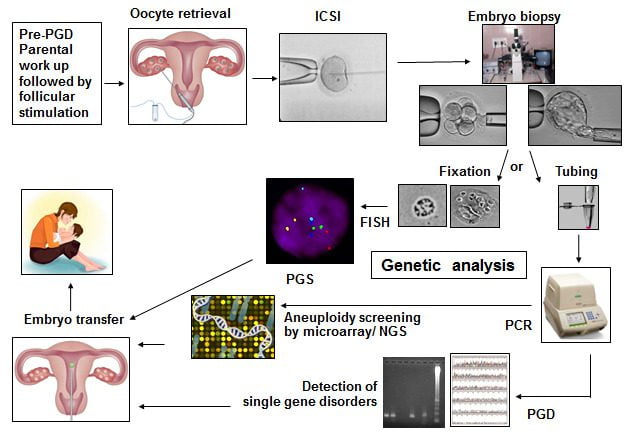
Steps involved in the PGT cycle:
For PGT testing, multiple embryos are developed by performing ICSI. The steps involved in PGT are:
- Pre-PGT work-up:
For the couple opting for PGT for single gene disorders (PGT-M), it is important to carry out Genetic testing for the disorder in both the partners prior to PGT-M. This determines the mutation (alteration in genetic material) status of both partners. Based on the genetic report, the actual PGT protocol is developed. PGT for single gene disorders (PGD/PGT-M) is carried out only for the known disorder and mutation which is identified for the couple. Other unknown genetic abnormalities cannot be tested at this time.
Other important genetic tests for PGT:
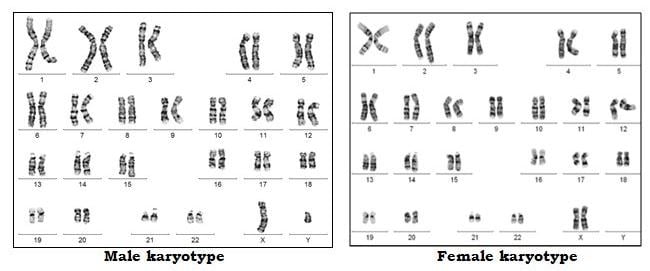
1. Karyotyping: Chromosomal analysis is carried out to check for any aneuploidy or translocation or presence of mosaicism.
2. Sperm FISH to check for a percentage of aneuploid sperm. (i.e. sperm with an abnormal number of chromosomes).
3. Sperm DNA Fragmentation Indiex to check for the percentage of sperm with DNA fragmentation.Many routine blood parameters are also tested. Once these reports are ready, the ovarian stimulation cycle begins.
- Hormonal stimulation and oocyte retrieval:The female partner undergoes ovarian stimulation using hormones in order to obtain adequate number of eggs. The eggs are collected under anesthesia.
- ICSI/ IMSI: ICSI (Intracytoplasmic sperm injection) is performed. A single sperm is injected into the cytoplasm of the mature egg. After fertilization, the embryo is further incubated in culture till Day 5/Day 6/Day 7.

- Embryo biopsy at the Blastocyst stage:For chromosomal aneuploidy screening (PGT-A), embryo biopsy is generally performed on Day 5 or Day 6 (Blastocyst stage). For single gene disorders (PGT-M) the embryo biopsy is performed on Day 5 or Day 6 (Blastocyst Stage).
The Blastocyst is made up of a cluster of cells called the Inner Cell Mass (ICM): which forms the fetus and the trophectoderm cells (which form the placenta). By gentle micromanipulation about 5-8 trophectoderm cells are aspirated into a pipette, loaded into the tube and sent for genetic analysis.
All of the above steps are carried out in the Embryology laboratory. The trophectoderm cells are then transported to the Genetics Lab for further testing. After biopsy, the embryos are cryopreserved till the day of embryo transfer.
- Different techniques of genetic testing include Fluorescence in Situ Hybridization (FISH), Array Comparative Genomic Hybridization (aCGH) and Next Generation Sequencing (NGS).
- Frozen Embryo Transfer (FET) of the genetically normal embryos is carried out and sometimes in the same cycle by doing a Quick Run Analysis in a subsequent cycle.
- A pregnancy test is performed 14 days later.

Please note that our centre does not perform any form of sex determination by PGT in any form.
Objectives of PGT:
- Prevention of chromosomally abnormal births for couples having a history of failed fertilization after IVF-ICSI, missed abortions or for carriers of balanced translocations
- To increase the chances of implantation
- Reducing the incidence of spontaneous miscarriages
- Reduction in multiple offspring
- Eliminates the risk of being affected with a familial gene disorder.
- Savior sibling (HLA matched) to cure a previously affected sibling with cord blood stem cells.
Risk and Limitations:
Even though the benefits of PGT-M/PGT-A are considerable, some risks and limitations have to be kept it mind. This procedure cannot guarantee a healthy pregnancy or eliminate the risk of miscarriage, stillbirth or the birth of a child with an abnormality.
- If less number of oocytes are retrieved, the ICSI cycle may have to be repeated.
- Occasionally, there may be decreased fertilization, few healthy embryos or embryos that cleave slowly and do not reach the Blastocyst stage. Hence a biopsy may not be possible.
- If the quality of the embryo is poor, the genetic material present in the biopsied cells may be degraded causing breaks in the cellular DNA. Such DNA material may not give results. In such a case, a repeat trophectoderm biopsy may be needed.
- It is possible that all the embryos may show genetic abnormalities and hence embryo transfer may not be possible.
 A blastocyst is an embryo that consists of more than 100 cells and forms 5 days after fertilization. Using sophisticated culture media, we can select embryos that remain healthy in culture and reach the blastocyst stage prior to transfer. A higher implantation rate has been observed following transfer of blastocysts. Currently our practice is to transfer 1 to 2 embryos at blastocyst stage. The extra embryos are then frozen by vitrification. In case of less number of good quality embryos, a Day 3 transfer of 2 embryos can be performed.
A blastocyst is an embryo that consists of more than 100 cells and forms 5 days after fertilization. Using sophisticated culture media, we can select embryos that remain healthy in culture and reach the blastocyst stage prior to transfer. A higher implantation rate has been observed following transfer of blastocysts. Currently our practice is to transfer 1 to 2 embryos at blastocyst stage. The extra embryos are then frozen by vitrification. In case of less number of good quality embryos, a Day 3 transfer of 2 embryos can be performed.
We achieved the first pregnancy in India using the technique of Laser Assisted Hatching and Blastocyst Transfer (LAHBT) in 2000.
 Treatment with ovulation induction at the time of Assisted Reproduction produces many oocytes. We cryopreserve extra embryos for future cycles. Our freezing protocol is by vitrification. All embryos are coded, labeled and stored in special containers to maintain their identity. We have an active oocyte vitrification program. Oocyte cryopreservation is carried out prior to chemotherapy and in women who want to delay childbearing.
Treatment with ovulation induction at the time of Assisted Reproduction produces many oocytes. We cryopreserve extra embryos for future cycles. Our freezing protocol is by vitrification. All embryos are coded, labeled and stored in special containers to maintain their identity. We have an active oocyte vitrification program. Oocyte cryopreservation is carried out prior to chemotherapy and in women who want to delay childbearing.
The process of Vitrification and the process of thawing has to be very precise to ensure survival of the oocytes and embryos.
Our IVF Centre has installed the Cryogatt Freezing System which is a Safety net for freezing Embryos, Sperm and eggs using Artificial Intelligence & Radiofrequency Identification so that there is no mixup of samples.
We are the first IVF Centre in Asia to have installed this system.
All of these biological materials are stored at -196 degrees Centigrade and can be indefinitely stored. The samples are placed in straws or vials that are either bar coded or labelled manually. One has to be very careful to avoid mix up of biological samples. Sometimes the labels can become unsticky. In such cases identification of the biological sample can become difficult. Also the correctly labelled straw has to be identified and removed from the other samples in less than 15 seconds. Any longer exposure can damage the biological material. The Cryogatt System bypasses all these difficulties.
How does the Cryogatt System work?
The Cryogatt System has Radiofrequency Identification that is safe for humans.
Each straw is tagged with a RF Identifier (RFID). A platform containing the software program is placed on the rim of the cryostorage tank. As the straw is being removed, the program’s tagging system identifies the straw and the Reader displays the patient’s name ensuring the right sample is being thawed. This also prevents inadvertent thawing of other samples thereby preventing any human error.

For more information click here

Semen Cryopreservation and Banking
We routinely have a back-up semen sample frozen for couples who are undergoing treatment in case of inability to give a semen sample on the day of the IUI, IVF or ICSI. Men undergoing orchidectomy/cancer treatment prior to radiation and chemotherapy can also avail of our cryopreservation facilities. Those undergoing ICSI are encouraged to freeze their sperm so that we have adequate number of sperm at the time of ICSI. We routinely cryopreserve testicular and epididymal sperm, so that repeated attempts at obtaining fresh epididymal and testicular sperm are avoided.
Donor Insemination Program
We follow all the guidelines of the ART Act of India and the Indian Council of Medical Research (ICMR). We have a tie up with a sperm bank for donor semen. This has undergone stringent evaluation. The donors are tested for HIV, Hepatitis B and C and VDRL. The semen quality is ensured by following the WHO criteria. Karyotyping of the Semen Donor is carried out. Specific Genetic Tests can be performed if requested by the couple.
 Infertility and its treatment cause significant stress to the couple. This is detrimental to the reproductive cycle. Before definitive treatment begins, we encourage couples to talk about their stress factors and initiate counseling. We have one of the largest series on psychiatric screening and counseling for ART and many other studies cite our work in this field. Dr. Rajesh Parikh, Consultant Neuropsychiatrist and his team of counsellers will guide you through your cycle.
Infertility and its treatment cause significant stress to the couple. This is detrimental to the reproductive cycle. Before definitive treatment begins, we encourage couples to talk about their stress factors and initiate counseling. We have one of the largest series on psychiatric screening and counseling for ART and many other studies cite our work in this field. Dr. Rajesh Parikh, Consultant Neuropsychiatrist and his team of counsellers will guide you through your cycle.
We have counselled more than 10000 infertile couples.
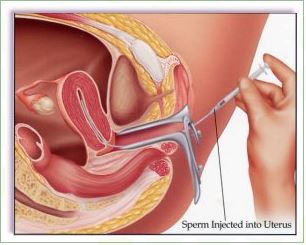
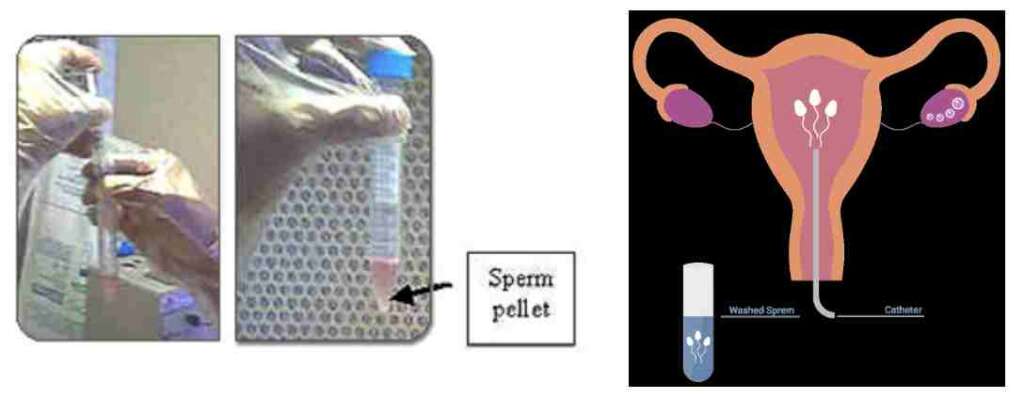
Intrauterine Insemination: IUI
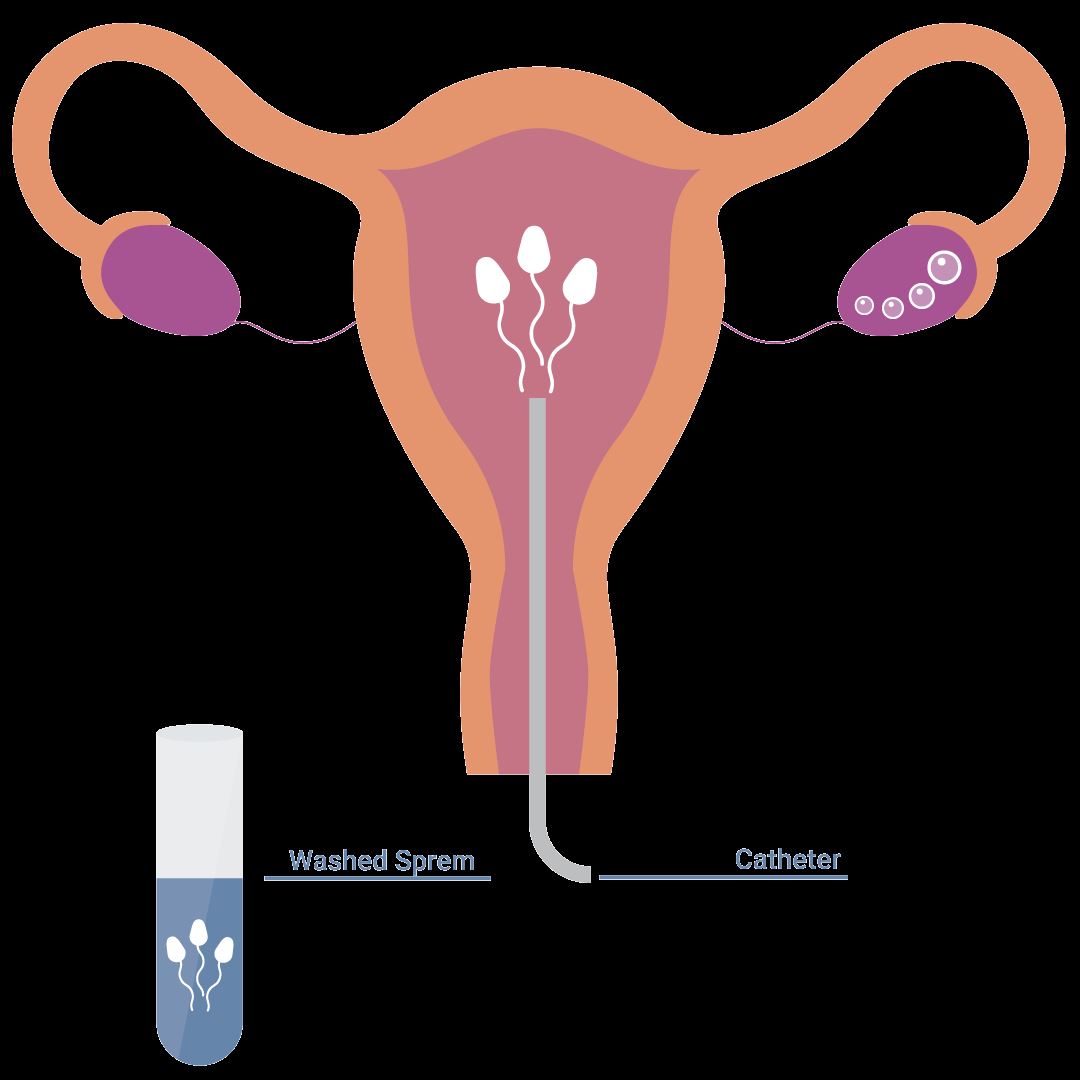
Intrauterine Insemination (IUI) is a fertility enhancing procedure in which the ejaculated semen is washed free of seminal plasma and other debris, concentrated into a small volume of highly motile sperm, and is then injected into the uterus as close to the fallopian tubes as possible, in an attempt to achieve a pregnancy. The purpose of IUI is to increase the number of sperm that reach the fallopian tubes and thus increase the chances of fertilization. IUI provides the sperm an advantage by giving it a head start but still requires the sperm to reach and fertilize the egg on its own. It is a less invasive and less expensive option compared to In Vitro Fertilization.
When is IUI used?
Male Factor Indications
- Marginally low sperm count
- Decreased sperm motility
- Increased number of abnormal sperm (abnormal morphology)
- Disorders of sperm function, such as increased sperm DNA fragmentation
- Defects of the penis, e.g., hypospadias or severe penile curvature
- Retrograde ejaculation or other forms of ejaculatory dysfunction, e.g. patients with spinal cord injury needing electro-ejaculation
- Sexual dysfunction, premature ejaculation
Female Indications
- Poor cervical mucous with a poor post coital test
- Persistent cervicitis
- Cervical stenosis
- Endometriosis
- Ovulatory dysfunction
- Psychological or physiological sexual dysfunction
Common Indications
- Unexplained infertility
Indications for Donor IUI
- Azoospermia with spermatogenic failure
- Previous vasectomy not amenable to IVF/ICSI /TESA/PESA
- Previous cancer therapy with radiation or chemotherapy.
Contraindications for IUI
- Severe male infertility
- Tubal Disease
- Moderate to severe endometriosis
Fertility Drugs for Intrauterine Insemination (IUI)
- Clomiphene Citrate Letrozole
- Gonadotropins
- IUI can be done in a natural cycle also
How does IUI work?
Before intrauterine insemination, ovulation-stimulating medication can be used, in which case ultrasound monitoring will be necessary to determine when the eggs are mature. The IUI procedure is performed around the time of ovulation, typically about 24-36 hours after the surge in LH hormone that indicates ovulation will occur soon or 36 hours after the hCG trigger.
The semen sample is washed in the lab to separate the semen from the seminal fluid. A catheter is used to insert the sperm directly into the uterus. This process maximizes the number of sperm that are placed in the uterus, thus increasing the possibility of conception. There are different techniques of sperm preparation such as sperm Migration and Swim up, Overlay, Double Gradient Centrifugation (Dgc), MACs, Microfluidics technology.
The IUI procedure takes a few minutes and involves minimal discomfort. A pregnancy test is done 14 days after the IUI.
Success Rates with IUI
Success rates with IUI depend upon the procedure being performed
- For the correct indications
- Avoiding the performance of IUI when contraindications exist
- The age of the woman
- Sperm Parameters
By and large, birth rates per cycle of IUI performed for the correct indications are reported to be about
- 15% for women under the age of 30
- 12% for women ages 30 to 35
- 7% to 8% for women ages 35 to 39
- Less than 2% for women over the age of 40.